


Wrist Fractures
WHAT ARE WRIST FRACTURES?
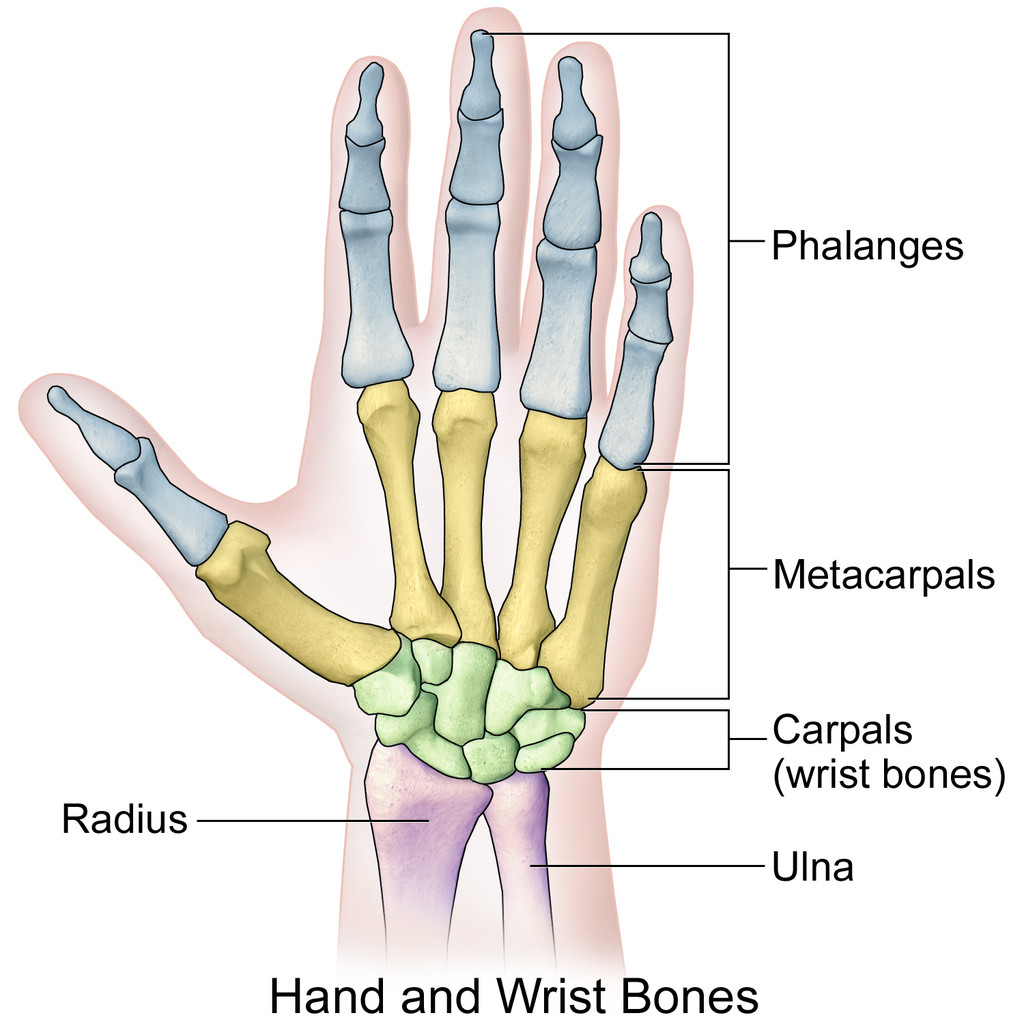
The skeleton of the wrist consists of two bones, the radius and the ulna. In wrist fractures, the most frequently broken bone is the radius, so it is more academic to talk about distal radius fractures.
CAUSES
They usually occur in older people with osteoporotic disease after falls from their own height, however, high energy injuries such as traffic accidents or contact sports are a frequent cause of distal radius fractures in young patients.
SYMPTOMS
Pain, hematoma, deformity, shortening or abnormal position are the usual signs.
DIAGNOSIS
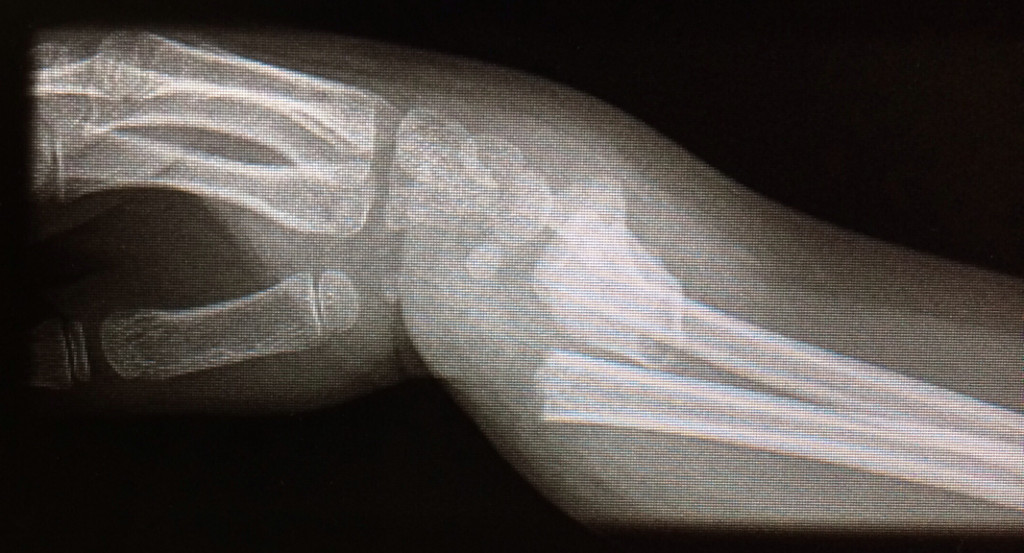
Physical examination and x-rays are essential for the accurate diagnosis of these fractures and guiding treatment. Standard radiographs can be supplemented by a CT scan in cases of intra-articular fractures.
TREATMENT
It is important to differentiate extraarticular fractures (those that respect the radiocarpal joint) from articular fractures (in which the fracture line affects the articular cartilage). Orthopedic treatment: If the fracture is not displaced, the bone is of good "quality", and it is extra- articular: the indicated treatment can be done by immobilization with plaster for 5-6 weeks. If the fracture is displaced and / or the bone quality is poor, surgery is indicated. This operation will aim to "reduce" the wrist and place an osteosynthesis system to keep the bone in place. There are several methods of osteosynthesis, the most common are:
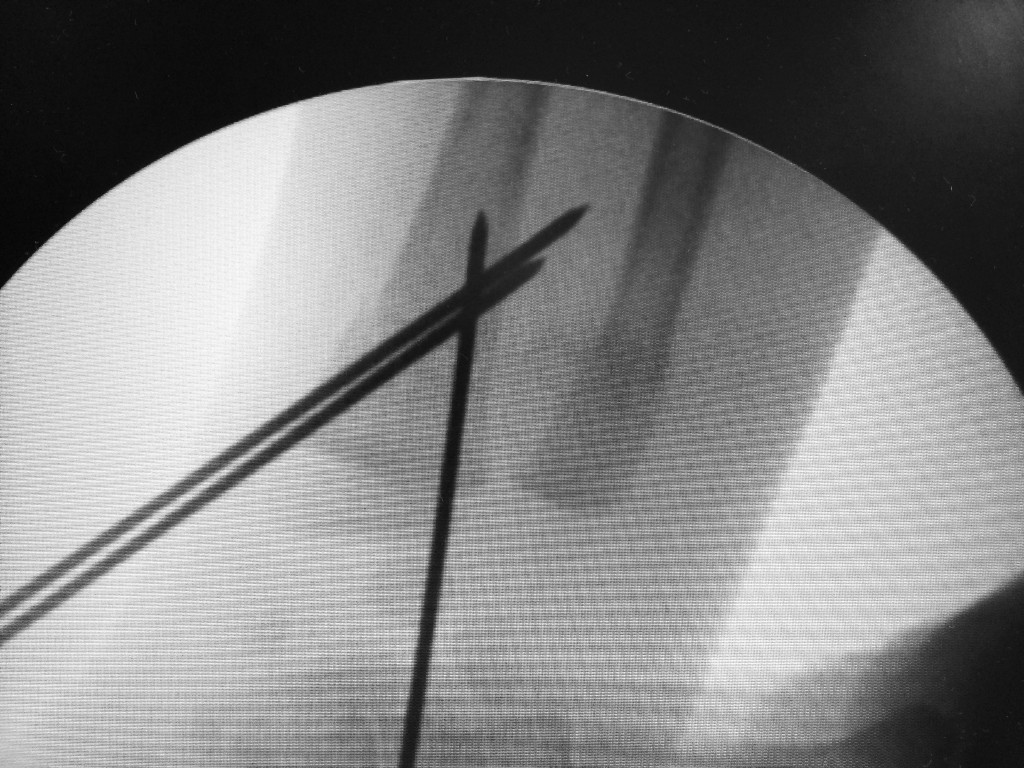
- Synthesis with needles: After reduction of the fracture, 1.5 mm needles are used to maintain the
fracture reduction during 5 weeks. From that moment on, the safe extraction of the needles can be
carried out and the mobilization started.


- Reduction and synthesis with screw: some fractures can be treated with this method but it is
mandatory to add a plaster.




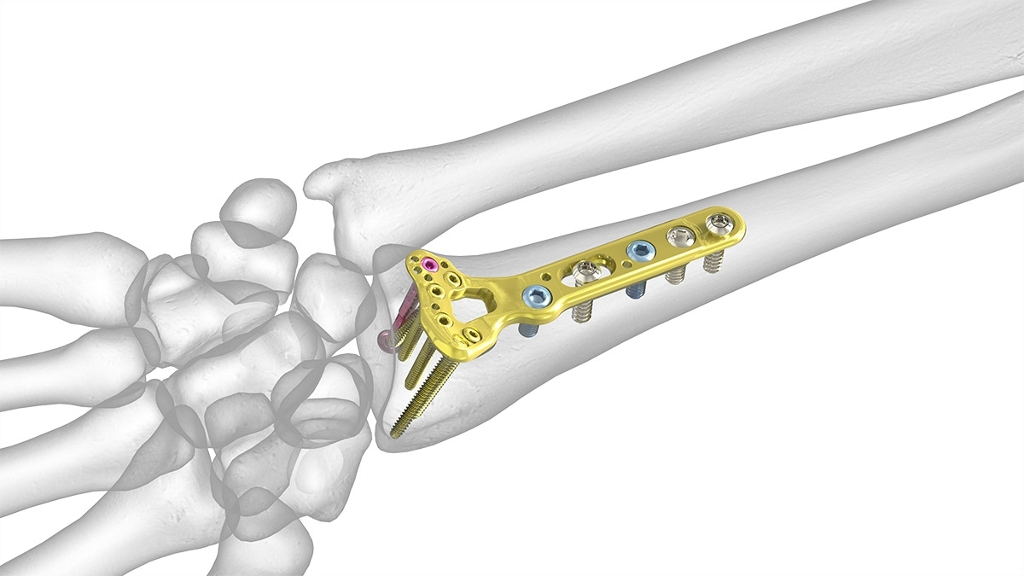
- Osteosynthesis with plate: this is the most used technique. Through a small palmar incision in the
wrist, and after reduction of the fracture's fragments is done, we fixed it with a plate and screws.
This technique allows a perfect reduction of the fracture obtaining the best results. In the case of
intra-articular fractures it may be necessary the complementary use of arthroscopy to assist the
fracture and prevent joint steps. The use of a plate allows early mobilization since the day of the
procedure without the need to use a plaster.
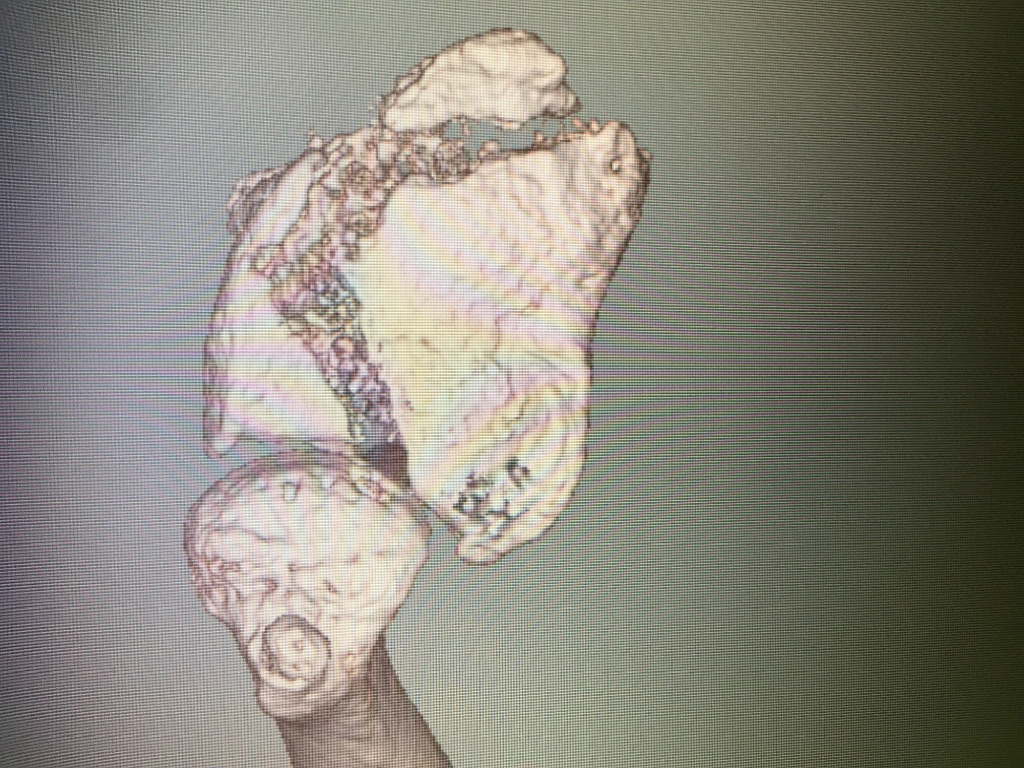
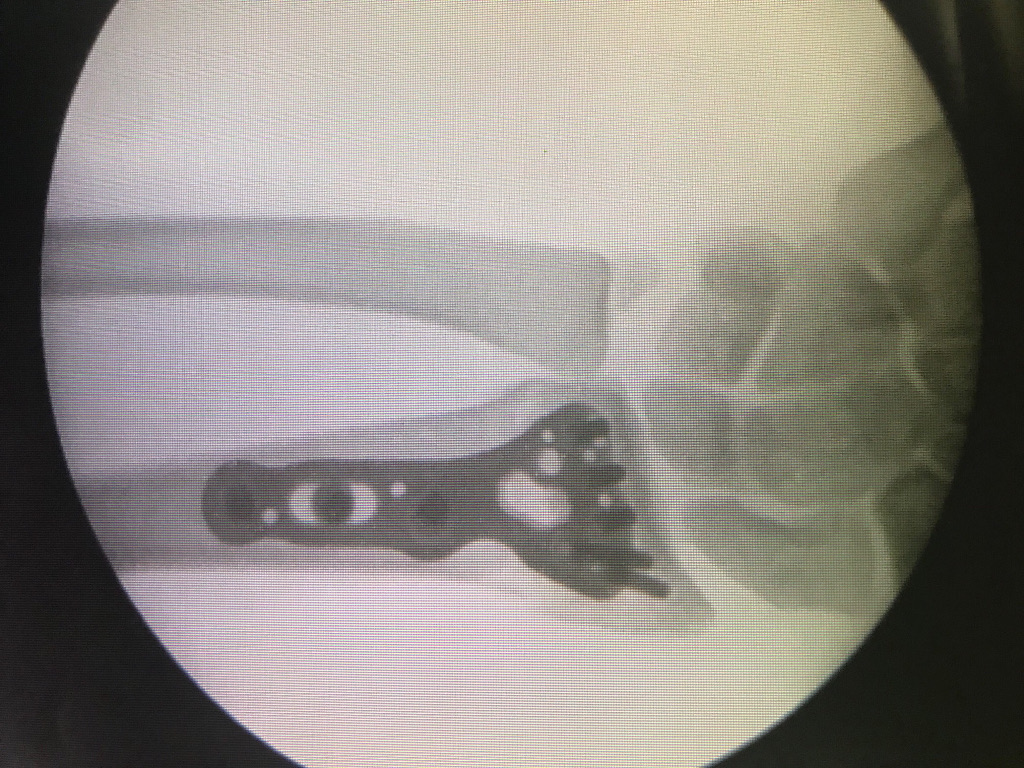
- Case 1 (fractura de radio distal intraticular tratada con placa)


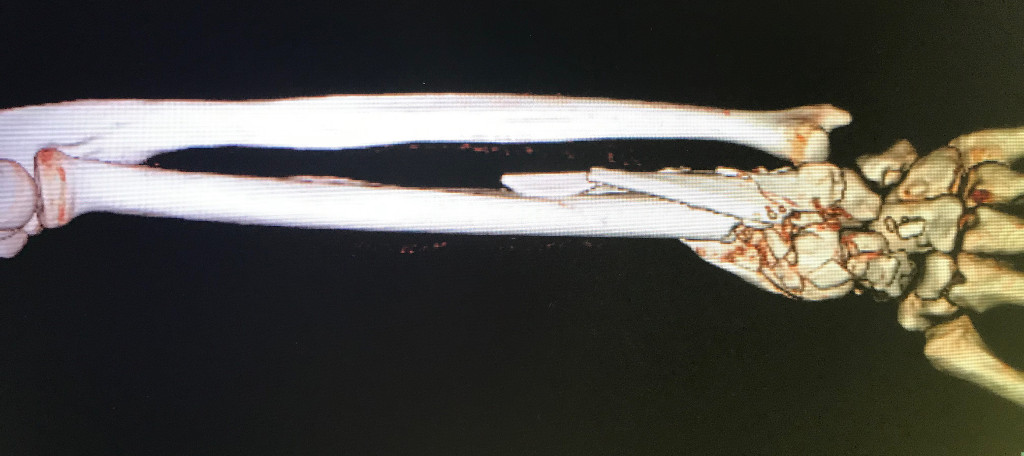
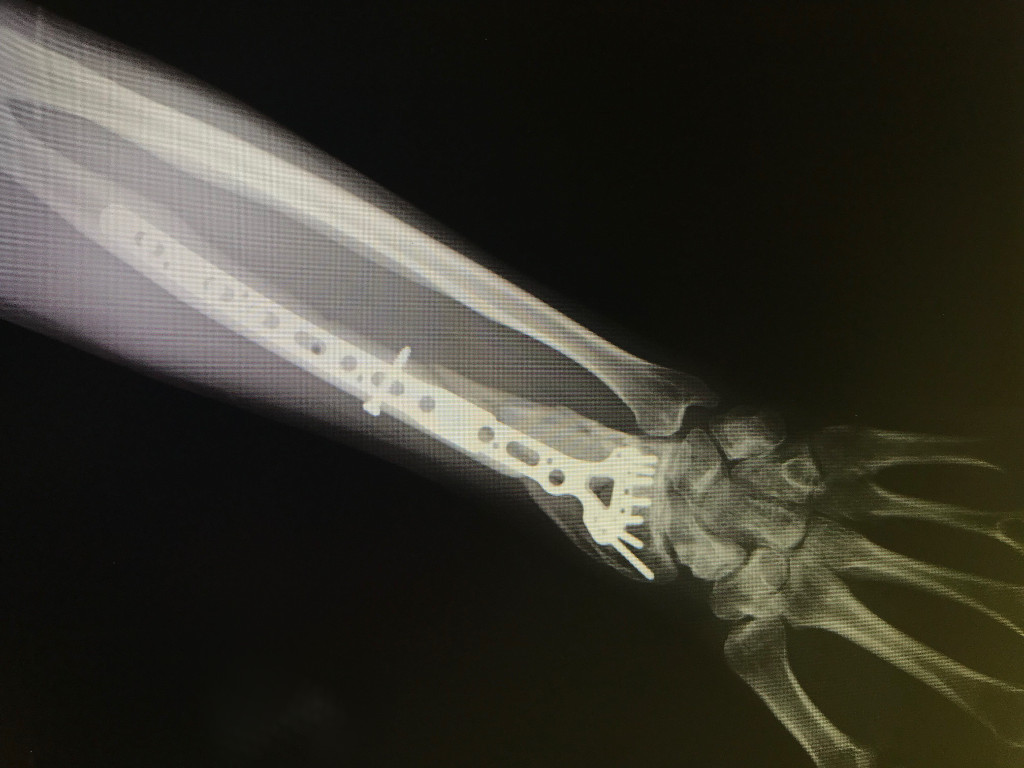
- Case 2 (fractura conminuta de radio tratada con placa larga)
Scaphoid Fracture
INTRODUCTION
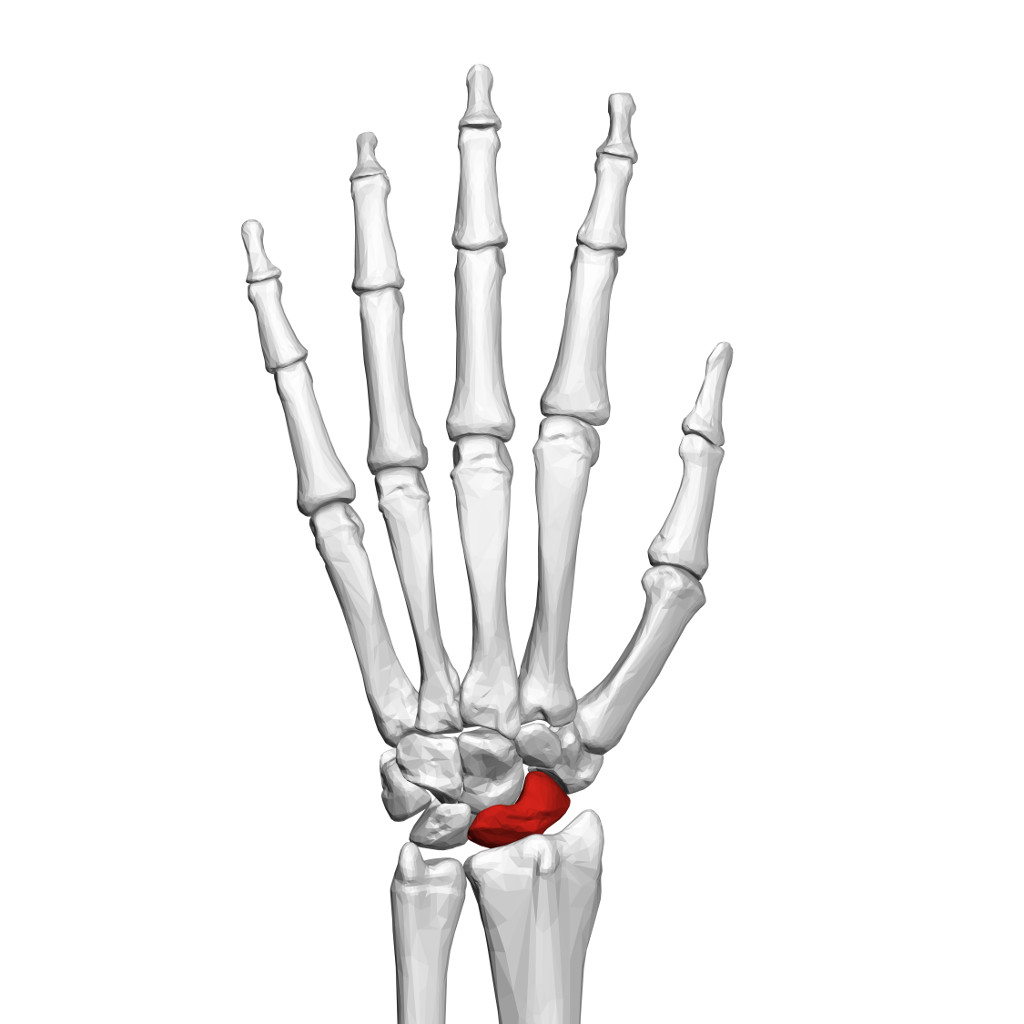
The wrist is formed by the two bones of the forearm (the radius and the ulna) and eight small carpal bones. The carpal bones are arranged in two rows at the base of the hand. The scaphoid bone is one of the carpal bones on the thumb side of the wrist, just above the radius. The bone is important for both motion and stability in the wrist joint. Scaphoid fractures account for 70-80% of all carpal bone fractures.
CAUSES
The usual mechanism is falling on an outstretched hand with resultant hyper-extension of the wrist or purely compressive force. Occasionally stress fractures are also encountered although these are less common, and only usually seen in athletes (shot-putters or gymnasts).
SYMPTOMS
Symptoms of a scaphoid fracture typically include pain and tenderness in the area just below the base of the thumb ("anatomic snuffbox"). These symptoms may worsen when you try to pinch or grasp something.
DIAGNOSIS
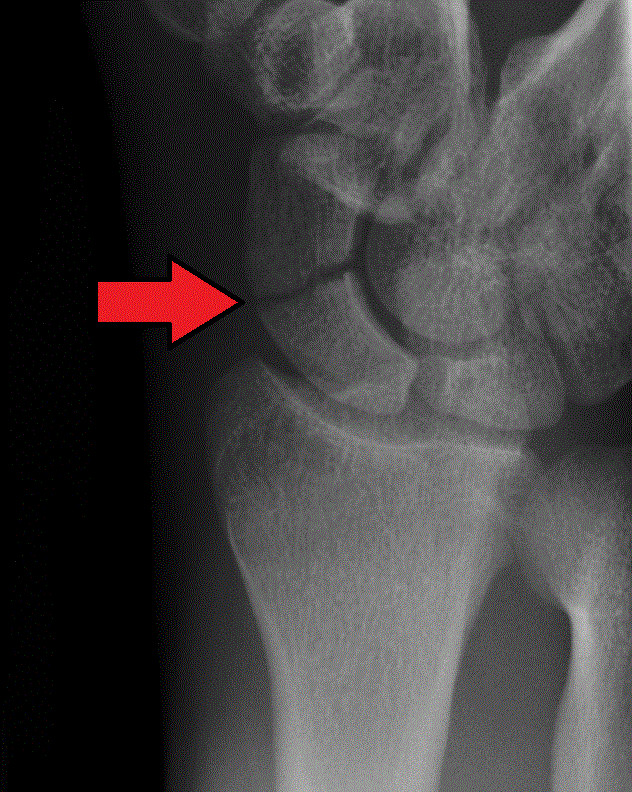
Scaphoid fractures are diagnosed by X-rays however, a non-displaced fracture does not show up on an X-ray when it is taken as early as the first week. In this cases or in displaced fractures, an MRI, or a CT scan can also be ordered to confirm the diagnosis of the scaphoid.
TREATMENT
If the fracture is non-displaced, it could be treated by immobilization in a cast. The cast usually covers the forearm, hand, and thumb. Although the fracture may heal in as little as 8 weeks, the healing can often be delayed. One reason for this delay is the variable blood supply to different parts of the scaphoid bone. The fracture can disrupt the bone's blood supply, impairing the healing. In these patients, screw fixation surgery (by a percutaneous approach) should be recommended to avoid prolonged casting. If the fracture is displaced, surgery is more likely to be recommended. Simple, minimally displaced fractures may be better managed with a small operation through a 0,5 mm incision of the wrist to place a screw across the fracture and compress the fragments together. The advantage of this is that the rate of fracture healing is slightly higher and that patient doesn't need to wear a splint.

Wrist arthroscopy
INTRODUCTION
Wrist arthroscopy is a minimally invasive procedure that allows the surgeon to diagnose and treat the disorders of the wrist by using small incisions (portals) and instruments. Wrist arthroscopy continues to grow in popularity as a feasible adjunct in the management of disorders of the wrist. The procedure enables evaluation and detection of carpal structures under bright magnifying conditions with minimal morbidity as compared with arthrotomy.
INDICATIONS
It allows the visualization of the cartilage surfaces of all bones in the wrist and better evaluation of the ligaments between the various bones of the wrist. Initially wrist arthroscopy was used as a diagnostic tool to confirm ligament, cartilage tears, or inflammatory processes. Now many of these problems are also treated arthroscopically. The indications includes synovial biopsies or debridements, repair of the triangular fibrocartilage complex (TFCC), stabilization procedures for ligament disruptions and carpal instabilities, removing ganglion stalk, reducing distal radius fractures, and removing bone fragments or loose bodies.
TECHNIQUE
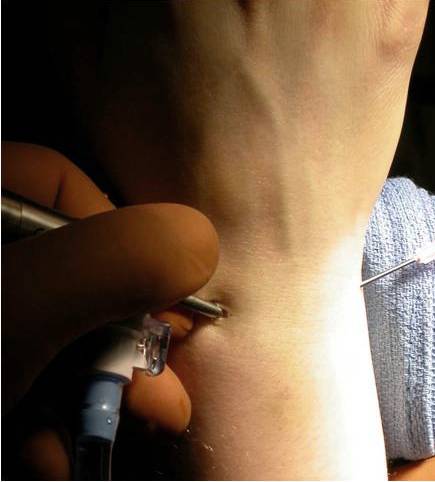
Wrist arthroscopy is a minimally invasive procedure in which a lighted tube less than 2mm in diameter connected to a camera is placed into the wrist joint by using small incisions in the skin (about 5mm long). The camera lens magnifies and projects the small structures in the wrist onto a television monitor, allowing for more accurate diagnosis. The wrist is usually distracted and fluid is infused into the joint to expand the joint and allow improved visualization during the procedure.
ADVANTAGES
The advantages of arthroscopic surgery over traditional surgery include:
- Smaller surgical incisions which result in less scarring and a lower infection rate
- Less trauma to tissues
- Less pain and a quicker recovery period
- Earlier mobilization following surgery
- A shorter hospital stay
